If I want more cash control, private pay usually wins. If I want steadier trip volume, Medicaid usually wins. That’s the short answer.
Here’s what matters most:
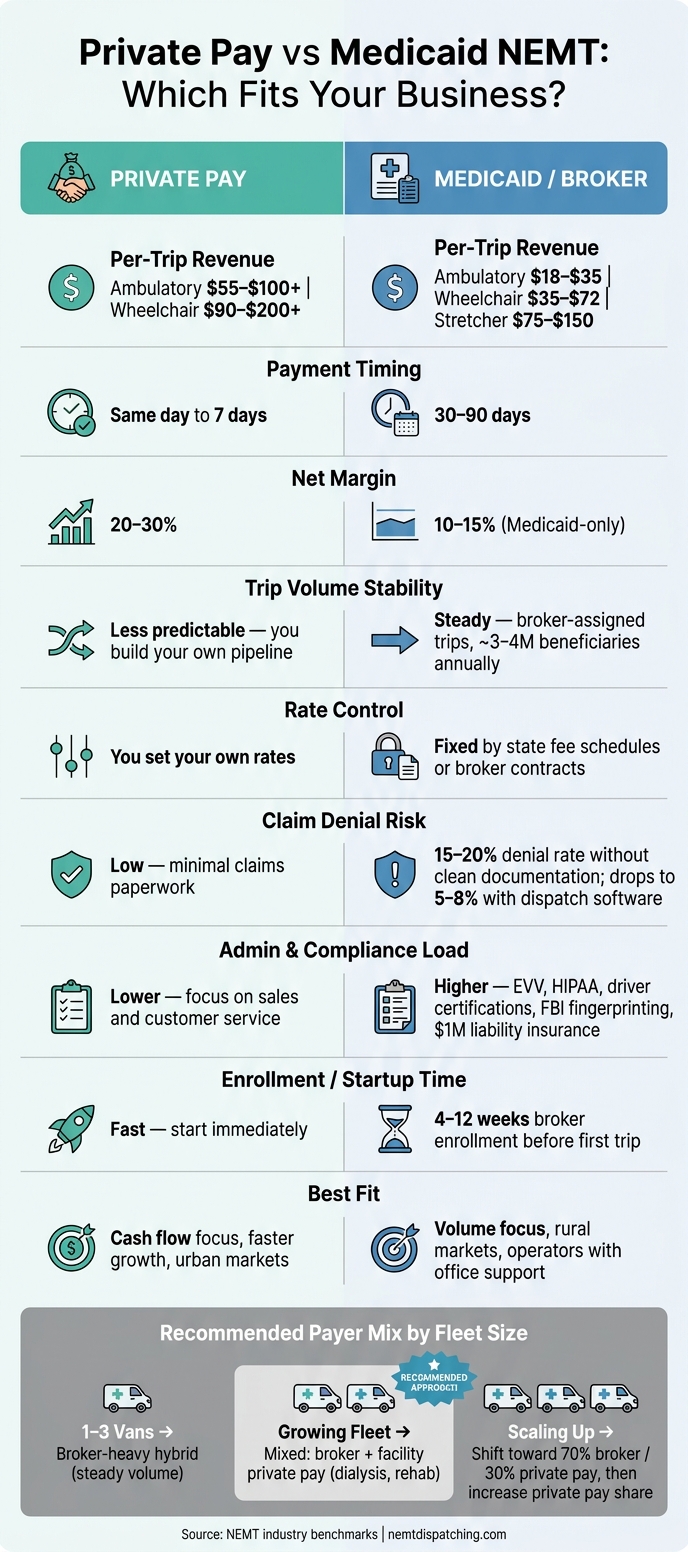
- Private pay trips often bring in 30%–50% more per ride
- Private pay is often paid the same day or within 7 days
- Medicaid can take 30–90 days to pay, and manual dispatch vs. software choices impact how quickly you can resolve those billing delays
- Medicaid brings built-in demand through brokers
- Private pay gives me control over rates, service area, and trip types
- Medicaid comes with more paperwork, claim rules, and denial risk while requiring strict HIPAA compliance for all patient data
- Many small and mid-size fleets do best with a mixed model
So if I’m running 1–3 vans, I’d usually look at a broker-heavy mix first for trip flow, then add private pay accounts for better margins. If I already have office staff, cash reserves, and clean billing, Medicaid can fill the schedule. If I need cash in the door faster, private pay can be the better fit.
Private Pay vs Medicaid NEMT: Side-by-Side Business Comparison
Which Insurance Providers Pay for NEMT | NEMT Business Education | RouteGenie
sbb-itb-af83355
Quick Comparison
| Criteria | Private Pay | Medicaid |
|---|---|---|
| Who pays | Rider, family, or facility | State Medicaid or broker |
| Rate control | I set rates | Rates are fixed |
| Trip volume | Less steady | More steady |
| Payment timing | Same day to 7 days | 30–90 days |
| Admin load | Lower claims work | Higher paperwork and billing work |
| Sales need | High | Lower |
| Best fit | Cash flow and margin focus | Volume and broker trip flow |
My takeaway: pick the model that fits my cash flow, office capacity, and local demand – not just the one that sounds better on paper.
Medicaid NEMT: Steady Trip Volume, Fixed Rates, and Higher Compliance Demands
Medicaid trips move through broker and plan networks, which usually means steadier ride volume but less control for the operator. About 3–4 million Medicaid beneficiaries use NEMT each year, so demand is built in. That’s a big plus.
But volume is only part of the story. The day-to-day reality comes down to broker rules, heavier paperwork, and slower cash flow behind each trip.
How Medicaid Contracts, Brokers, and Reimbursement Work
In most states, Medicaid trips don’t come straight from the state. They’re usually routed through managed care plans or brokers. Big names like ModivCare and MTM handle a large share of trip assignments and distribute rides to providers inside their networks.
The trade-off is simple: you get access to steady trip flow, but you don’t get much say over pricing. Reimbursement is set by state fee schedules or broker contracts, so rates are fixed in a way that private-pay operators don’t have to deal with. Rates change by state and broker, but this table gives a useful benchmark.
| Service Level | Typical Medicaid Base Rate | Billable Miles |
|---|---|---|
| Ambulatory | $18–$35 | $1.50–$2.50 |
| Wheelchair | $35–$72 | $2.00–$3.50 |
| Stretcher | $75–$150 | $2.50–$4.00 |
Getting into a broker network also takes time. Enrollment often runs 4–12 weeks before your first trip is assigned.
Administrative Demands That Affect Small Fleets
This is where Medicaid can get heavy for small fleets.
Starting out means meeting a long list of compliance rules: commercial auto liability coverage of around $1 million per occurrence, ADA-compliant vehicles, driver background checks, FBI fingerprinting, drug testing, CPR/First Aid certification, and HIPAA training. That’s a lot before the first passenger even gets in the vehicle.
Then the trip-level paperwork starts. Each ride usually needs the date, time, pickup and drop-off addresses, patient name, Medicaid ID, mileage, and a patient or caregiver signature. Many states also want EVV and GPS proof that the trip happened as billed.
If any of that is missing or wrong, claims can get denied at rates in the 15%–20% range. And there’s another catch: brokers don’t pay for empty miles. So if your routing is sloppy, your margins can disappear fast.
That’s why Medicaid tends to fit operators who have enough cash on hand and enough office support to deal with denials, payment delays, and constant follow-up. For a small fleet, the admin load can matter just as much as the trip count.
How Dispatch Software Can Help With Medicaid Operations
Once you’re running more than a few vehicles, handling Medicaid paperwork by hand gets messy fast.
Tools like NEMT Cloud Dispatch can automate scheduling, dispatching, billing, fleet management, and GPS tracking, which helps keep trip records cleaner and claims easier to support. In Medicaid, clean claims matter because small documentation mistakes can hit revenue hard.
When trip logs, GPS records, and signatures are tracked in a more organized way, denial rates can drop from the 15%–20% range to about 5%–8%. That kind of shift can make a plain business difference, especially when fixed reimbursement rates leave little room for error.
Those controls become even more important when Medicaid is stacked up against private pay.
Private Pay NEMT: More Pricing Control, but Less Predictable Demand
Private pay flips the Medicaid setup. You’re not waiting for broker-assigned trips. You set your own rates and win customers directly. That can mean better margins, but demand is less steady. You feel that most in pricing, trip volume, and cash flow.
How Private Pay Revenue and Pricing Differ From Medicaid
With private pay, you control your rate sheet. Ambulatory trips often range from $55 to $100+, while wheelchair trips usually fall between $90 and $200+. Many providers also charge add-on fees for wait time, after-hours service, holidays, or special equipment.
Payment timing is also different. In many cases, money comes in at the time of service or within 7 to 30 days, instead of the 30 to 90 day reimbursement window that many Medicaid operators deal with. For a small fleet trying to cover payroll and fuel, that faster payment cycle can make a big difference.
A common setup is a base rate plus a per-mile fee. Some operators also test subscription-style bundles for recurring rides, such as dialysis trips, to smooth out revenue from week to week.
Building Customers and Meeting Service Expectations
Higher rates sound great on paper. But they only work if your vehicles stay busy. In private pay, demand doesn’t show up on its own. You have to build it.
The clearest path to steady trip volume is referral work. That means building relationships with:
- Hospital discharge planners
- Rehab facilities
- Dialysis centers
- Senior living communities
- Case managers
These referrals matter because private pay has no built-in trip pipeline. Even five to 10 recurring dialysis patients can give you a steady base of revenue. In established NEMT companies, recurring transport clients make up 65% to 70% of revenue.
Private pay riders also expect more from the service. They want on-time pickups, clear communication, clean vehicles, and a polished experience. That’s not extra. That’s what helps justify the higher rate. Strong Google Business Profile reviews can also help you show up when local families or facilities search for a ride provider.
With Medicaid, the broker owns most of the client relationship. With private pay, that relationship is yours. So is the pressure that comes with it.
How Software Supports Private Pay Scheduling and Billing
As private-pay volume grows, admin work can pile up fast. Repeat scheduling and manual invoicing often become the first pain points.
A platform like NEMT Cloud Dispatch can help automate recurring trip scheduling, GPS tracking, invoicing, and facility account management. That kind of setup helps when you’re juggling repeat riders and multiple facility accounts at once.
Sending a clean invoice to a senior living facility the same day a trip is completed is the kind of detail that keeps recurring accounts organized and builds long-term client trust.
Private Pay vs Medicaid: A Direct Comparison for Owners and Dispatchers
The payment model affects staffing, cash flow, and working capital. For owners and dispatchers, that means this choice goes way beyond billing. It changes how the business runs day to day.
Revenue, Cash Flow, and Margin Trade-Offs
Once you understand how each model works, the big issue becomes simple: which one helps cash flow without burying your team in extra work?
The clearest gap comes down to per-trip revenue and how fast you get paid. Private pay is often collected at the time of service or within 7 days. Medicaid reimbursements usually take 30 to 90 days, which means operators need enough working capital to cover payroll, fuel, and other bills while they wait. That delay can put pressure on a small company fast.
Margins show the same pattern. Medicaid-only operators usually land in the 10–15% net margin range. Operators using a mixed payer model can reach 20–30%. In plain terms, broker volume can keep vans moving, but private pay can give you more room to breathe.
| Feature | Medicaid / Broker | Private Pay |
|---|---|---|
| Payment Timing | 30–90 days | Immediate to 7 days |
| Net Margin | 10–15% | 20–30% |
Operations, Staffing, and Documentation Burden
The money side matters, but the daily workload matters too. And this is where many operators feel the difference.
Every Medicaid trip requires tight documentation. That includes patient ID, pickup and drop-off times, exact addresses, trip purpose, vehicle and driver IDs, and signatures. On top of that, drivers may need certifications such as PASS training, CPR/First Aid, and HIPAA compliance to meet broker contract rules.
That admin load isn’t small. New operators often deal with 15–25% claim denial rates until their billing process is cleaned up and consistent. One missing detail can slow payment or kill a claim altogether. Private pay cuts down much of that claims work, but it shifts the pressure elsewhere. You spend less time fixing denials and more time handling sales, service, and client communication.
| Task | Medicaid | Private Pay |
|---|---|---|
| Staffing Focus | Billing and compliance | Sales and customer service |
| Scheduling | 48–72 hours advance notice required | Flexible, same-day possible |
Which Model Fits Your Business Stage, Market, and Fleet Size
This trade-off makes more sense when you line it up with your fleet size and market.
For startups with 1 to 3 vehicles, broker volume is usually the first move. It brings steady trip volume and gives you time to build a compliance record before you take on the sales and marketing work that private pay demands. That can be a smart way to keep the lights on while learning the business.
As the fleet grows, many operators add facility-based private pay accounts like dialysis centers, rehab clinics, and senior living communities. That mix can steady revenue without walking away from the broker volume that keeps vehicles full.
Market type matters too. Rural markets often lean toward Medicaid because long-distance mileage reimbursements help make up for lower base rates. Urban markets often lean toward hybrid or private-pay models because higher trip density cuts deadhead miles and makes routing more efficient. For many growing companies, a common goal is a 70/30 split: 70% broker volume for stability and 30% private pay for margin, then shifting that mix over time.
| Scenario | Recommended Model | Key Reason |
|---|---|---|
| Startup (1–3 vans) | Broker-heavy hybrid | Immediate volume helps cover fixed costs |
| Growing fleet | Diversified with facility contracts | Recurring dialysis and rehab trips help stabilize revenue |
| Urban market | Hybrid or private pay focus | High density supports efficient routing and direct pricing |
| Rural market | Medicaid / broker | Long-distance mileage supplements help offset lower base rates |
| High-growth goal | Hybrid, shifting toward private pay | Higher margins improve cash flow |
The next move is to choose the payer mix that lines up with your cash flow, staffing setup, and local demand.
Conclusion: Choosing Medicaid, Private Pay, or a Hybrid Model
Once you stack up trip volume, margins, and office work, the choice usually comes down to two things: your local market and your cash position.
Medicaid tends to work best when you want steady trip volume. Private pay gives you more control over pricing and usually gets cash in the door faster. A hybrid model sits in the middle. You can lean on Medicaid broker trips for baseline volume, then use private pay trips to add better margins.
Before you change your payer mix, track the numbers that tell the real story: cost per trip, claim denials, and vehicle utilization. If those numbers are off, growth can turn into a headache fast.
Before you choose, test these five factors:
- Medicaid market access and pricing: Are brokers still taking new providers, or is the market already crowded? What are local Medicaid rates for wheelchair and ambulatory trips? Rates can vary by more than 300% between states.
- Private market demand: Are there dialysis centers, nursing homes, or hospital discharge planners nearby that can send recurring private pay trips? Referrals and local search visibility matter a lot here.
- Billing and office capacity: Medicaid means keeping Driver Qualification Files up to date, dealing with EVV compliance, and working denied claims. For a small team, that can be a heavy lift.
- State approval or licensing requirements: Does your state require extra operator approvals before you can take Medicaid trips?
- Cash flow position: Can you cover 60–90 days of payroll, fuel, and insurance before Medicaid pays? If not, private pay or a mixed model can ease that strain.
NEMT Cloud Dispatch can help manage scheduling, billing, and trip records across both payer types.
Start with the mix your current fleet, market, and cash flow can handle, then adjust as demand and margins change.
FAQs
How much cash reserve do I need for Medicaid?
Because Medicaid reimbursement often takes 30 to 90 days, a Medicaid-focused NEMT business needs enough working capital to pay for fuel, maintenance, and driver wages while waiting for that money to come in.
A common rule of thumb is at least $10,000 per vehicle.
At the company level, most startups should plan for $30,000 to $50,000 in available capital, plus extra cash reserves to handle day-to-day operating swings.
When should I switch to a hybrid model?
Consider a hybrid model if you need steadier cash flow and better margins. Medicaid-only operations often run on thin 10%–15% margins, with payment cycles that stretch from 30 to 90 days.
Bringing in private pay and facility contracts can change the math. These jobs can deliver 20%–30% margins and payments in 1 to 7 days. That faster money coming in can help balance Medicaid rate caps, regional differences, and rising operating costs.
Cloud-based NEMT software can help too. It makes multi-payer billing easier, which matters when you’re juggling different contract types and payment timelines.
Which model is better for a small fleet?
For a small fleet, the best fit is usually a mixed payer model. Medicaid can bring steady, high-volume trip demand. Private pay, on the other hand, often brings faster cash flow and more revenue per trip.
That balance matters. Many small fleets use Medicaid for routine, predictable rides and then fill open time slots with higher-margin private pay work. It’s a practical way to keep vehicles busy without leaning too hard on just one source of revenue.
Reliable cloud-based NEMT software can help here too. It makes it easier to handle different billing setups, stay organized, and improve route profitability.