
If I were starting a NEMT business today, I’d focus on permits, Medicaid enrollment, insurance, and cash flow before buying a van. The market is large – about $9.5 billion a year and 55 million trips annually – but new operators often get stuck on licensing delays, claim denials, and slow payment cycles.
Here’s the short version:
- Start with the paperwork first. Business setup, NPI, Medicaid enrollment, broker approval, and local permits can take 30 to 90+ days.
- Keep cash on hand. I’d plan for 60 to 90 days of fuel, payroll, and insurance before the first Medicaid payment lands.
- Choose the right service mix. Most small fleets start with wheelchair-accessible vehicle (WAV) service because it can cover both ambulatory and wheelchair trips and often pays more than ambulatory-only work.
- Watch the math. One WAV often costs about $30,000 to $55,000 to put on the road, with monthly costs near $5,800.
- Tight paperwork matters. New operators can see 15% to 25% claim denials from missing or bad trip records, while clean systems can push that below 5%.
- Growth comes later. Broker trips can fill the schedule first. After that, facility contracts and private-pay work can help margins.
A NEMT company is not just a driving business. It’s a compliance, billing, and scheduling business with vehicles attached. If I wanted to avoid early mistakes, I’d make sure the rules, trip types, fleet plan, driver files, and billing process all line up before launch.
| Area | What matters most |
|---|---|
| Business setup | LLC or corporation, EIN, bank account, local permit rules |
| Payer access | Type 2 NPI, Medicaid enrollment, broker credentialing |
| Fleet plan | Ambulatory, WAV, stretcher, vehicle age and mileage limits |
| Insurance | Commercial auto, general liability, workers’ comp, abuse/molestation coverage |
| Driver files | MVR, background check, drug test, CPR/First Aid, PASS |
| Billing | Authorizations, odometer logs, signatures, HCPCS coding, EDI claims |
| Growth | On-time rate, denial rate, trips per vehicle, accounts receivable days |
Bottom line: I’d treat NEMT as a cash-flow and rule-heavy business from day one. Get approved first, buy for the trips you can bill, and build a clean trip-to-claim process before trying to add more vehicles or contracts.
sbb-itb-af83355
How the NEMT Business Model Works
NEMT is scheduled medical transportation for medically stable patients who can’t drive or don’t have a way to get to care. The driver’s job is transportation, not medical treatment. Demand tends to stay steady because many trips repeat week after week, especially for dialysis, specialist visits, and hospital discharges. That’s why your service mix has such a big effect on revenue.
Who Uses NEMT and What Trips You Will Actually Run
Most NEMT companies operate across three main service levels: ambulatory, wheelchair (WAV), and stretcher.
Ambulatory trips are for patients who can walk on their own. WAV trips are for manual or power wheelchair users, so you need a van with a lift or ramp. Stretcher trips are for patients who can’t sit upright, such as people going home after surgery.
For many operators, WAV is the most common place to start. It serves a larger billable market than ambulatory service and usually pays more per trip. Dialysis runs are a big part of that picture because they often repeat three times per week. Behavioral health visits and specialist appointments can help fill open slots in the schedule.
Average Medicaid rate benchmarks for common trip types are below:
| Service Level | Avg. Medicaid Rate/Trip | Vehicle Needed | Best Fit For |
|---|---|---|---|
| Ambulatory | $15–$35 | Standard sedan or minivan | Patients who walk independently |
| Wheelchair (WAV) | $30–$75 | Accessible van with lift/ramp | Manual or power wheelchair users |
| Stretcher | $65–$150 | Stretcher-equipped van | Patients who cannot sit upright |
| Bariatric | $75–$180 | Reinforced WAV or stretcher van | Patients over 300 lbs |
Those rates don’t mean much if your fleet doesn’t match the trips you’re offered. A van that can’t handle the request is just missed revenue.
How Medicaid, Brokers, Facilities, and Private Pay Revenue Work
Medicaid is the main payer for most NEMT trips. In many states, brokers like Modivcare, MTM, and Southeastrans handle provider networks and send trips to local operators.
Broker work is often the fastest way to get volume on the board. The tradeoff is simple: broker rates usually land on the lower end of the pay range. Direct contracts with dialysis centers, hospitals, or skilled nursing facilities can pay more and give you a steadier calendar, but they usually want proof that you can perform, including 98%+ on-time performance. Private pay trips can bring in 30%–50% more than Medicaid rates, and payment often comes in faster.
A practical way to build the business is to start with broker contracts, build volume, and stack cash reserves. After that, you can add facility contracts and private-pay trips to improve margins as the company gets more stable.
Startup Costs and Basic Unit Economics
Getting one WAV into service usually costs $30,000–$55,000 total. A used wheelchair-accessible van that’s 3–5 years old usually runs $22,000–$38,000, and commercial auto insurance for a WAV often costs $5,000–$8,000 per year.
Typical monthly operating costs for one vehicle come to about $5,800:
| Monthly Operating Cost Category | Typical Cost |
|---|---|
| Driver Wages (W-2) | $3,200 |
| Fuel | $600 |
| Insurance Payment | $750 |
| Software/GPS | $260 |
| Maintenance Reserve | $250 |
| Total Monthly Ops | $5,800 |
To cover that expense level, an operator usually needs about 10–14 ambulatory trips per day or 5–9 WAV trips per day, depending on reimbursement rates.
Early on, two numbers matter more than almost anything else: deadhead miles and denial rates. Deadhead miles eat into margins because you’re driving without pay. Denial rates hurt cash flow because the trip happened, but the claim doesn’t get paid. New operators often deal with denial rates of 15%–25% due to paperwork mistakes. Billing software or a billing service that knows NEMT can bring that number below 5%. Choosing the right NEMT dispatch software features is critical for automating these claims and reducing errors. Medicaid usually pays 14–30 days after a clean claim, so every avoidable denial slows down cash coming in.
That math only works when intake is clean, dispatch is tight, and claims go out right the first time. From there, the next step is understanding how trips are dispatched, documented, and paid.
How to Set Up a Compliant NEMT Company
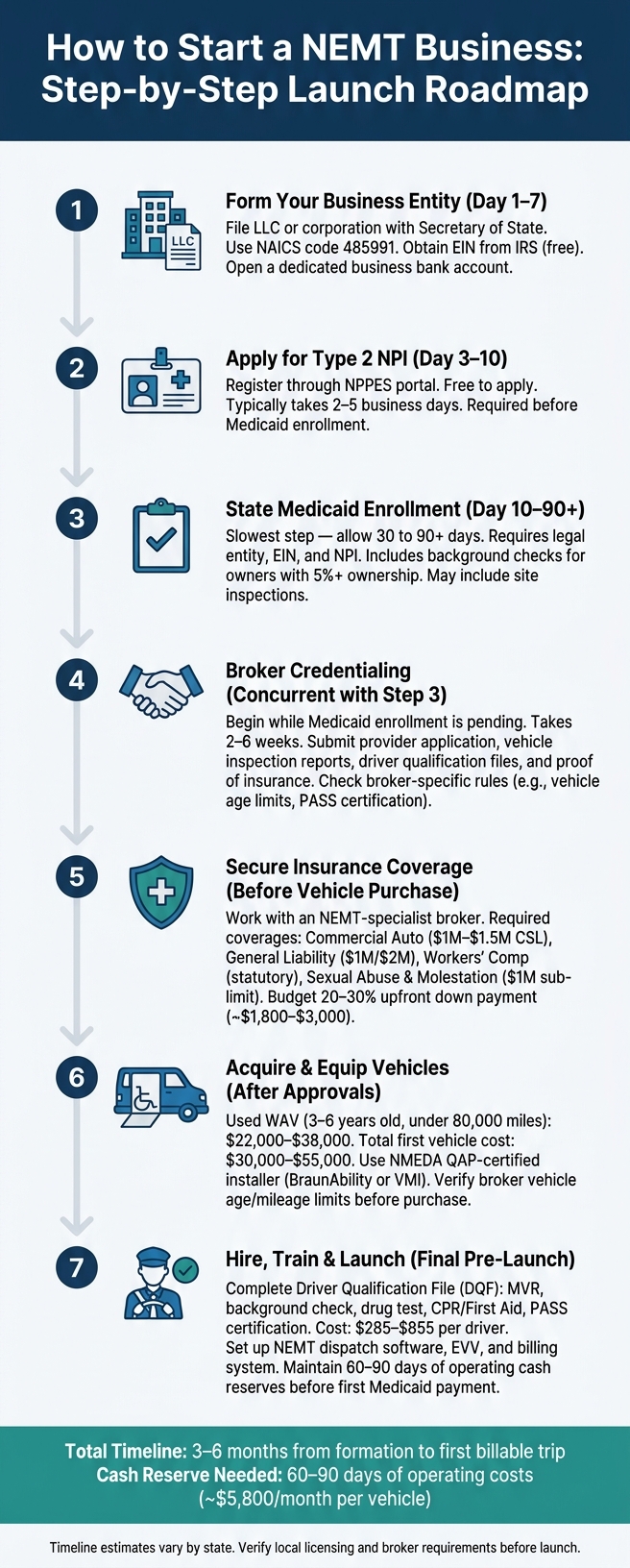
How to Start a NEMT Business: Step-by-Step Launch Roadmap
Getting the legal and admin setup right decides whether you can bill, get paid, and keep contracts. If the paperwork isn’t in place, you won’t get payer access, you can’t submit claims, and revenue stalls. In most cases, the setup takes 3–6 months from start to first trip. These filings are the gatekeepers for enrollment, credentialing, and billing.
Business Formation, Licensing, and Tax Registration
Start by forming an LLC or corporation with your Secretary of State. That step separates personal and business liability, which matters when vehicle accidents or patient incidents can lead to large claims. Use NAICS code 485991 (Special Needs Transportation) on your filings.
After the entity is formed, get your Employer Identification Number (EIN) from the IRS. It’s free. Then open a business bank account dedicated to the company so you can receive Medicaid EFT deposits.
You’ll also need to check state, county, and city rules for transportation permits. Costs vary a lot. Licensing fees range from $0 in states like Texas and Florida to $1,500 in New York. California requires a CPUC TCP permit and DOJ Live Scan fingerprinting. Minnesota requires MnDOT certification before you can operate. It’s smart to verify these rules before you buy vehicles, not after.
Set aside 60–90 days of operating cash for fuel, driver pay, and insurance before the first Medicaid payment shows up.
Medicaid Enrollment, NPI, and Broker Credentialing
The usual order is simple: form the business, get the EIN, and then apply for a Type 2 NPI through the NPPES portal. NPI registration is free and usually takes 2–5 business days.
Next comes state Medicaid enrollment, and this is often the slowest part. Expect 30–90 days or more. You’ll need your legal entity, EIN, and NPI. The process also includes criminal background checks for owners with 5% or more ownership, and it may include site inspections.
While Medicaid enrollment is still pending, begin broker credentialing. That step usually takes 2–6 weeks. Brokers ask for provider applications, vehicle inspection reports, driver qualification files, and proof of insurance.
One thing catches many new operators off guard: brokers often set tougher rules than the state minimum. Some won’t accept vehicles older than 10 years. Others ask for certifications like PASS. Check those rules before you purchase vehicles.
Once approvals are in place, your vehicle mix and onboard equipment decide which trips you can actually take.
Insurance, ADA, Driver Screening, and Compliance Checklists
Work with an insurance broker that handles NEMT coverage. A plain commercial auto policy often leaves gaps, especially for riders tied to wheelchair-assisted boarding and sexual abuse and molestation coverage. There are only about 30 carriers nationwide that write this risk class.
| Insurance Type | Typical Requirement | Estimated Annual Cost |
|---|---|---|
| Commercial Auto Liability | $1M–$1.5M CSL | $4,500–$15,000 |
| General Liability | $1M occurrence / $2M aggregate | $900–$3,500 |
| Workers’ Compensation | Statutory limits | $800–$6,000 |
| Sexual Abuse & Molestation | $1M sub-limit | $400–$2,000 |
Plan for an upfront insurance down payment of 20%–30% of the annual premium. That usually lands around $1,800–$3,000 when you first bind coverage. Dash cameras and telematics may cut premiums by 5%–15% with many carriers.
Before any driver takes a first trip, they need a complete Driver Qualification File (DQF). That file includes:
- A motor vehicle record (MVR) with no DUI in the past 7 years
- A criminal background check
- A pre-hire drug test
- CPR/First Aid certification
- A PASS (Passenger Assistance Safety and Sensitivity) certificate
Total credentialing cost per driver is typically $285–$855, depending on the state and the certifications required.
You also need a monthly screening process for every employee and contractor against the OIG List of Excluded Individuals/Entities (LEIE) and SAM.gov. Miss even one monthly check, and the contract can be terminated right away.
For ADA compliance, vehicles must meet 49 CFR Part 38 standards. That includes a minimum 600 lb lift capacity and a 4-point wheelchair securement system. If you use a ramp, the maximum slope is 1:4.
NEMT providers are HIPAA Business Associates and must maintain HIPAA compliance in NEMT operations. That means you need BAAs with software and billing vendors, and patient data should be encrypted with AES-256.
After compliance, the next gate is making sure the fleet matches the trips you want to run.
Vehicles, Equipment, and Safety Standards
After licensing and broker credentialing, the next hurdle is fleet readiness. If the vehicle or onboard setup is wrong, trips can get blocked before dispatch even begins.
Choosing Vehicles for Ambulatory, Wheelchair, and Stretcher Trips
Your fleet mix shapes almost everything: which trips you can take, which brokers will approve you, and how fast you earn back what you spent on vehicles. Ambulatory units help you handle more low-cost rides. WAVs open up the broadest compliant market. Stretcher units are often tied to higher-paying facility work.
For many startups, a used WAV is the best first move because it can handle both ambulatory and wheelchair trips. That kind of flexibility matters when you’re trying to keep the schedule full. Ambulatory sedans and minivans work well for rural routes and one-driver operations. Full-size rear-entry WAVs usually cost $28,000–$45,000 used and can fit larger power chairs and multi-passenger runs. Stretcher vans are built for facility transfers and bariatric loads, which sit at the top reimbursement tier.
| Vehicle Type | Body Style | Best Fit |
|---|---|---|
| Ambulatory Sedan/Minivan | Standard sedan or minivan | Rural routes, solo starts |
| WAV Minivan (Side-Entry) | Accessible minivan with ramp or lift | Urban/suburban mixed loads |
| WAV Full-Size (Rear-Entry) | High-roof van with rear lift | Power wheelchairs, multi-passenger routes |
| Stretcher Van | Modified full-size van | Facility transfers, bariatric |
Many new operators buy used vehicles that are about 3–6 years old, and a lot of them aim for units with under 80,000 miles to keep upfront costs in check. But there’s a catch: broker limits. Major brokers like Modivcare and MTM often cap vehicles at 10 years old and 200,000–300,000 miles. So before you buy, check the exact rules in your state. A vehicle that barely fits today can age out faster than you’d think, and that can turn into an expensive mistake.
For WAV conversions, stick with a NMEDA QAP-certified installer like BraunAbility or VMI. That step isn’t just paperwork. It affects safety, broker approval, and future inspections.
The vehicle you choose also affects routing, trip volume, and downtime when repairs come up.
Lifts, Securement, Seating, and Required Safety Equipment
Once you’ve picked the vehicle type, the next issue is the equipment inside it. This is what decides which riders you can move safely and which trips you should decline.
Under 49 CFR Parts 37 and 38, accessible vehicles must meet federal accessibility rules, and brokers often want 1,000-lb-rated equipment. The federal minimum lift capacity is 600 lbs, but many brokers ask for 1,000 lbs so the vehicle can handle heavier power wheelchairs.
Ramps usually cost less and have fewer moving parts, so they make sense when you want lower repair risk. Lifts are the better fit for heavier chairs and bariatric loads. Ramp installs usually run $3,500–$9,500, while hydraulic lifts are more like $8,000–$18,000. You also need an interlock that stops the vehicle from moving while the lift or ramp is deployed.
Each wheelchair position must have a 4-point tie-down system that meets WC18/WC19 standards, along with lap and shoulder belts . Products like Q’Straint or Sure-Lok meet those rules. Securement hardware usually costs about $800–$2,500 per position, and each wheelchair securement strap must have a minimum capacity of 2,000 lbs per strap .
For riders who need more support on longer trips, transport seating can make a big difference.
Every vehicle also needs a basic safety kit on board at all times:
- A 2A:10B:C rated, 5 lb fire extinguisher in a secured mount
- An ANSI-compliant Class A first aid kit
- Three DOT-compliant reflective emergency triangles
- A biohazard spill kit for body fluid cleanup
- A seatbelt cutter within driver reach
- Wheel chocks for loading on inclines
Maintenance Schedules and Driver Safety Training
Even a compliant fleet can fall apart fast without tight inspections and trained drivers. Every day a vehicle is out of service means fewer completed trips and weaker on-time numbers.
Daily pre-trip and post-trip inspections are required under 49 CFR Part 396, and drivers must complete a DVIR after each inspection. Those checks cover tires, brakes, lights, and a working test of the wheelchair lift. ADA-compliant lifts also need quarterly lubrication and an annual load test, and that paperwork has to stay in the vehicle life file. Maintenance records must be kept for the life of the vehicle plus three years.
| Maintenance Interval | Key Service Items |
|---|---|
| Daily | DVIR sign-off, fluid top-off, lift deployment test |
| Quarterly | Battery test, ADA equipment lubrication, HVAC check |
| Every 3,000–5,000 miles | Oil and filter change, tire rotation |
| 6,000–12,000 miles | Brake inspection, tire alignment |
| Annual | Full safety inspection, lift load test, brake service |
Plan for $0.10–$0.15 per mile in maintenance costs, or about $200–$400 per month on higher-mileage vehicles .
Driver training matters just as much as the vehicle. Every driver needs PASS certification before taking a first trip. PASS is the standard passenger-assistance course for safe, sensitive transport. Courses usually cost $50–$100 online or $150–$250 in the classroom. On top of PASS, drivers need CPR/AED and First Aid training renewed every two years, defensive driving every 2–3 years, and annual HIPAA awareness training .
These certifications do more than check a box. They help cut rider incidents, support clean paperwork, lower claim denials, and protect broker performance scores.
With the fleet and drivers ready, the next step is trip scheduling and day-to-day control.
Day-to-Day Operations: Dispatch, Routing, and Billing
Once the fleet is licensed and staffed, the day-to-day job is simple in theory: move each trip from request to paid claim without errors. In practice, that means tight handoffs, clean records, and a system that doesn’t fall apart when the schedule gets busy.
Building a Standard Trip Workflow from Intake to Payment
A trip usually moves through the same path each time: request, eligibility check, scheduling, dispatch, documentation, claim, and payment.
Requests can come in through broker portals like Modivcare or MTM, through facility calls, or from direct private-pay bookings. Before a trip hits the schedule, confirm Medicaid eligibility and pull the prior authorization number. Then assign the ride based on the level of service – ambulatory, WAV, or stretcher – and send it to the right vehicle.
Each trip record needs a full paper trail. At a minimum, capture:
- Pickup and drop-off times
- Member ID for Medicaid trips or client ID for private-pay trips
- Prior authorization number
- Level of service
- Odometer readings
- Driver and vehicle ID
- Member or client signature
- No-show notes
This part matters more than many operators think. If the documentation is messy, billing gets messy fast. After the driver closes the trip, that trip data turns into a claim using the right HCPCS Level II codes. For example, A0130 applies to wheelchair van trips, while A0160 applies to per-mile ambulatory reimbursement. The claim is then sent through EDI 837P format. Clean claims usually pay in 14 to 30 days, and ERA 835 remits should be matched to claims weekly.
Typical Medicaid rates by code are shown below:
| HCPCS Code | Description | Avg. Medicaid Rate |
|---|---|---|
| A0100 | Non-emergency transport: Taxi | $15–$28/trip |
| A0130 | Non-emergency transport: Wheelchair van | $30–$75/trip |
| A0160 | Per mile – ambulatory | $0.85–$1.75/mile |
| A0200 | Per mile – wheelchair van | $1.25–$2.50/mile |
That workflow holds up only when dispatch, routing, and billing are connected instead of living in separate places.
Dispatch Software, Routing, and GPS Tracking for Small Fleets
A few trips a day can be managed with spreadsheets and phone calls. After that, things start slipping. Double-bookings happen. Broker updates get missed. Drivers take longer routes than they should. Deadhead miles stack up, and margin gets thinner.
NEMT software brings intake, routing, and billing into one flow. It can pull trip requests straight from broker portals, flag expired credentials or coverage gaps before a trip is assigned, and build claims from the same trip record, so staff doesn’t have to enter the same data twice. Real-time GPS tracking gives dispatchers a live view of where vehicles are, which makes rerouting easier when traffic or delays hit. Electronic Visit Verification (EVV) adds GPS-stamped timestamps and digital signatures automatically, cutting down on paper logs and backing up Medicaid billing.
| Feature | Spreadsheets/Phone | General Fleet Tools | NEMT-Specific Software |
|---|---|---|---|
| Trip Intake | Manual entry | Manual entry | Automated broker integration |
| Routing | Manual/Google Maps | Basic GPS | NEMT route optimization |
| Compliance | Manual folder tracking | None | Hard-lock credentialing alerts |
| Billing | Manual portal entry | None | Integrated EDI 837P claims |
| EVV | None | Basic GPS | HIPAA-compliant EVV with timestamps |
Small fleets usually pick from three lanes: low-cost scheduling tools, mid-range routing platforms, or more advanced systems that also handle billing and compliance. GPS telematics data can also lower commercial insurance premiums by 5% to 15% at renewal.
Once routing is in shape, the bigger problem usually becomes data control.
HIPAA-Aware Scheduling, Billing, Claims, and Denial Control
Every trip touches PHI, so scheduling and billing need tight access controls.
Use role-based access, unique logins, MFA, short auto-timeouts, and AES-256 encryption for stored and transmitted data. Encrypt stored data with AES-256 and transmitted data with TLS 1.3.
Before signing with any software vendor, billing service, or cloud storage provider, get a signed Business Associate Agreement (BAA). Any vendor handling PHI needs a signed BAA.
It also helps to run a weekly QA review before billing closes. Pull each unbilled trip and check that the authorization number, odometer readings, and signature are all there. The usual denial triggers are pretty plain:
- Missing authorizations
- Mileage gaps
- Expired driver credentials
Those issues are much easier to fix during weekly QA than after a denial lands. Billing services that focus on NEMT typically charge about 3% to 8% of collected revenue.
Once denials, access, and billing are under control, the next pressure point is utilization and contract quality.
Scaling the Business: Metrics, Contracts, and Long-Term Growth
Key Metrics That Show Whether the Business Is on Track
With dispatch, billing, and compliance in place, the next step is simple: check whether the fleet is growing at a profit.
Once dispatch and billing are steady, scale comes down to three things: utilization, denial rate, and contract mix. Track a small set of metrics every week, and move fast when something slips. Then review a monthly P&L to catch fuel, overtime, and maintenance creep before it turns into a bigger problem.
| Metric | Target Benchmark |
|---|---|
| Trips per vehicle per day | 8–12 |
| On-time performance | 98% |
| Denial rate | Under 5% |
| Days in accounts receivable | 35–45 days |
Use your current break-even volume to decide if the business can handle more contracts without putting stress on the fleet.
Winning More Contracts Without Overextending the Fleet
When the numbers show extra capacity and steady on-time performance, go after contracts that match the fleet you already have.
Dialysis centers are usually the best source of repeat volume. Patients often need transportation three times per week for the long haul, which gives you a steady, recurring schedule. That kind of routine work makes planning a lot easier.
After dialysis, focus on hospital discharge planners, assisted living facilities, and cancer treatment centers. These relationships can bring in better-margin work than broker-only volume. To get your foot in the door, put together a simple outreach packet with:
- A certificate of insurance
- Vehicle photos
- A clear list of service levels
- The geographic area you cover
Social workers and case managers want specifics. They need to know exactly what you can handle and when.
Key Takeaways for Launching and Running a Durable NEMT Operation
The simplest way to scale NEMT is to grow only after the workflow becomes repeatable.
A durable NEMT business scales in order: compliance first, workflows second, growth last. Operators that standardize trip workflows, onboarding, and maintenance tend to scale with fewer problems.
FAQs
How much cash do I need to start?
Startup costs for a NEMT business usually fall between $8,000 and $55,000, based on the size of your operation and the type of vehicle you use.
If you’re starting small with one vehicle, you may be able to get going for $8,000 to $15,000. A more common setup with a wheelchair-accessible van often lands in the $15,000 to $30,000 range. If you’re planning a larger operation with multiple vehicles, costs can climb to $45,000 to $55,000+.
It’s not just about buying the vehicle, either. You’ll also need to set aside money for insurance, licensing, permits, and working capital. That last part matters more than many first-time owners expect, especially if you’ll be billing Medicaid and need cash on hand to deal with payment delays.
Should I start with one WAV or an ambulatory vehicle?
For most new NEMT operators, it makes sense to start with one vehicle. That’s the route many owners take because it keeps costs under control while giving them time to build a client base and learn how day-to-day operations work.
A common starting point is a used ambulatory sedan or minivan, which usually costs around $15,000 to $25,000.
If you plan to serve riders who can get in and out on their own, an ambulatory vehicle is often the right fit. But if your market includes wheelchair users, a WAV can bring in more revenue. The tradeoff is the higher upfront cost, usually $30,000 to $55,000, along with extra compliance requirements.
How can I avoid Medicaid claim denials?
Avoid Medicaid claim denials by keeping complete trip documentation, staying compliant, and billing accurately from the start. A lot of denials come down to missing or partial records, and that’s the kind of problem you can prevent.
Your trip records should include:
- Patient Medicaid ID
- Pickup and destination addresses
- Trip purpose
- Vehicle and driver details
- Signatures
- Odometer readings
- Prior authorization numbers when required
It also helps to keep your Medicaid enrollment and credentialing active, make sure drivers meet qualification and training rules, and double-check HCPCS codes, prior authorizations, and claim details before you submit anything.